
The following are both my medical and scientific objections to the current slate of COVID-19 vaccines.
First, and foremost, with respect to my medical objection, I have personally been infected with COVID-19 during the past year. Multiple studies have demonstrated that natural immunities are more effective than vaccines at preventing re-infection (although some contrary studies do exist as well) and numerous studies demonstrate that SARS-CoV-2 antibodies likely persist for long spans of time – with several studies suggesting for a lifetime (1-7).
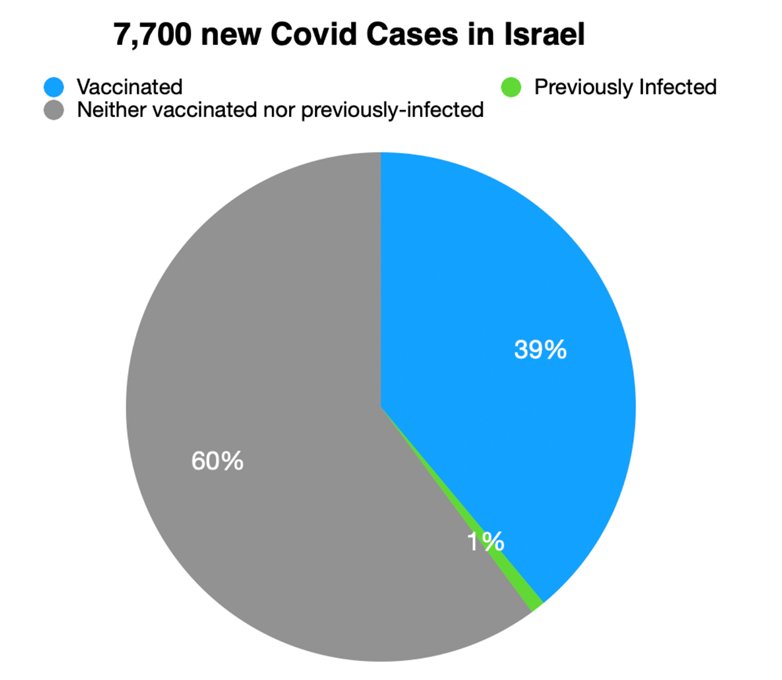
- Data out of Israel (N=7700) indicated that 40% of new infections were of previously vaccinated individuals while only 1% of their sample had a prior infection (suggesting better immunity from the natural infection) (See Figure 1).
- The Centers for Disease Control and Infection (CDC) reports that 74% of re-infected individuals reported on from a large social gathering in Massachusetts during July, 2021 were fully vaccinated, and 75% of patients requiring hospitalization from this sample were fully vaccinated (6). This demonstrates that vaccinations were clearly not helpful in preventing this disease.
- A preprint from the Department of Infectious Disease at the Cleveland Clinic reports on 52,238 employees of the Cleveland Clinic Health System in Ohio (8). They noted that for previously-infected people, the cumulative incidence of re-infection “remained almost zero.” According to the study, “Not one of the 1,359 previously infected subjects who remained unvaccinated had a [Covid-19] infection over the duration of the study” and vaccination did not reduce the risk. They concluded that “individuals who have had [Covid-19] infection are unlikely to benefit from COVID-19 vaccination.”
- Long-standing immunity has been seen in other virally-infected cohorts, including Spanish Flu survivors (9) and survivors of prior SARs/corona virus infections (10).
Further, some studies indicate that the experience of prior (non-SARS-CoV-2) viruses likely provide some degree of protection to those who have never been affected with COVID-19 (11, 12). In addition, there is research to suggest that natural infection may protect against variants of COVID-19 as well (13, 14). Ironically, some studies have indicated that vaccinations may have detrimental effects in those already experiencing COVID-19 (15). For example, there may be a risk of building tolerance to elements of the virus, which could actually decrease immune potency for those who have established natural immunity (15).
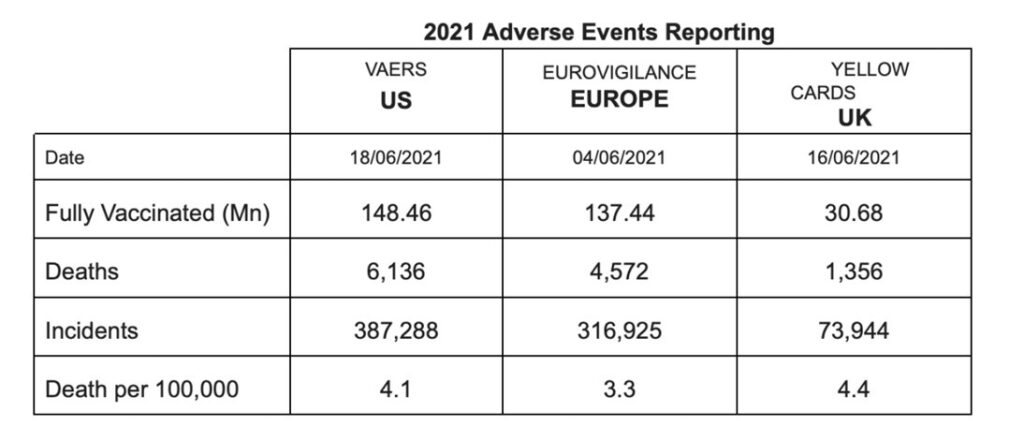
Second, there are significant science-based objections to the COVID vaccines. The fact is, that I have less than a 1 percent chance of dying from a COVID-19 infection and have already experienced this virus earlier this year. In contrast, the chance of experiencing an adverse effect of one of the commercially available vaccines is likely at least modestly higher for me (16). While the risk of either immediate adverse outcome is low, I believe the vaccines pose a greater personal risk to my safety due to the long-term unknowns associated with a new vaccination approach. The Vaccines Adverse Events Reporting System (VAERS) has demonstrated that the current slate of COVID-19 vaccines has a much higher rate of side effects (including death) than all vaccines combined over the past 30 years (See Table 1 and Figure 1 and the VAERS website – https://www.openvaers.com/covid-data). Overall, the rate of side effects associated with the SARS-CoV-2 vaccines remains fairly low, but this rate is higher than risk of death from COVID-19 for virtually all living individuals, and does not consider any unknown (and seemingly highly viable) long-term consequences. In fact, Dr. Robert Malone, an individual who contributed to the development of mRNA techniques has argued that creating spike proteins may not be harmless as is being claimed.
Every drug or vaccine is toxic at some level in some percent of people, and there’s pretty clear evidence that the spike protein expressed from vacinnes is causing toxicity in a small subset of patients. The question is, how big is that subset, and how broad and bad are those toxicities? The honest truth is, we don’t know. And furthermore, there’s a lot of signs that that information is being withheld from us.”
Dr. Robert Malone, co-developer of mRNA techniques
The available COVID-19 vaccines lack adequate research to insure their safety (particularly with regard to longer term effects), and this is bolstered by the published literature.
- None have long-term outcome data.
- The messenger RNA vaccines are a new technique in general, which has never been established for human use with regards to safety profile nor long-term outcome. Several unprecedented “firsts” have been introduced into this “rushed” process (16).
- These new vaccines do not operate in the same manner as past vaccines. Traditional vaccines involve the injection of a small amount of virus into the body in order to trigger a natural, immune response. In contrast, mRNA techniques introduce a synthetic mRNA material at the cellular level. (First to use mRNA technology against an infectious agent).
- Bill and Melinda Gates Foundation recently divided vaccines into three categories, including simple, complex, and unprecedented. The latter were defined as diseases for which there has never before been a suitable vaccine (for conditions like malaria or AIDs). Unprecedented vaccines are expected to take 12.5 years to develop and are believed to have a very low probability of success (i.e., less than 2% chance of success in a Phase III clinical trial)(17).
- It defies explanation, common sense, and any reasonable logic, that we now have an unprecedented vaccine developed in only 2 years, which we are to believe has an efficacy of 90-95%. [See critiques in British Medical Journal (18) and other references (16) by immunologists/scientists making exactly the same argument].
- First vaccines to use polyethylene glycol (PEG) in an injection.
- Mohamed et al. (2019) have described several negative findings regarding PEG and the immunological activation it has been shown to produce (including complement-based activation) (19, 20). In animal studies, complement activation has been demonstrated as a cause of both anaphylaxis and cardiovascular collapse, and PEG activates complement pathways in humans.
- Antibodies against PEG occur frequently in the general population.
- Lila et al. (2018) note that the “existence of such anti-PEG antibodies has been intimately correlated with an impairment of therapeutic efficacy in tandem with the development of severe adverse effects in several clinical setting employing PEGylated-based therapeutics.”
- Pre-existing antibodies to PEG have been linked to more common and more severe reactions upon re-exposure (21).
- Multiple studies have documented occurrences of anaphylaxis in persons exposed to PEG (22, 23), and anaphylactic reactions to mRNA vaccines have been widely reported in the media (16, 24).
- First time Moderna has ever brought any product to market (16, 25).
- First vaccine to have public health officials telling those who receive the vaccine to expect an adverse reaction (16).
- First to be implemented publicly with nothing more than preliminary efficacy data. There have been no standard and extended preclinical and clinical trials of the two mRNA vaccines.
- First coronavirus vaccine ever attempted in humans.
- First injection of genetically modified polynucleotides in the general population.
- These new vaccines do not operate in the same manner as past vaccines. Traditional vaccines involve the injection of a small amount of virus into the body in order to trigger a natural, immune response. In contrast, mRNA techniques introduce a synthetic mRNA material at the cellular level. (First to use mRNA technology against an infectious agent).
- Other concerning medical findings in first six months of SARS-CoV-2 vaccine reporting (14):
- The lipid nanoparticles, which are the carriers of the mRNA, were supposed to remain in the muscle but are showing up throughout the body, including the ovaries, the liver, and possibly the bone marrow. Long-term effects remain unknown.
- The spike-protein created by the vaccines appears to be capable of crossing the blood brain barrier and can create inflammation in the brain (26, 27).
- The rate of vaccine-related deaths in the first 6 months of available SARS-CoV-2 vaccines (6000+ deaths in the USA), exceeds that associated with all vaccines developed over the last 30 years combined. This finding is disturbing and deserves focused study. Of note, the number of deaths by the end of July had exceeded 12,000 (more than doubling in the last month). (See the VAERS reporting system: https://www.openvaers.com/covid-data).
- Negative data regarding the available vaccines are being underreported or outright suppressed (16) [also note that the counter arguments to vaccination that I am making are rarely seen in the media although they are clearly discussed in academic journals].
- The argument has been made that vaccines have been mandated in the past, but these have typically been well-established and followed an established, traditional technique/theory. Additionally, exemptions on both medical/personal and religious grounds have typically been recognized and upheld.
- The mandated use of such untried (experimental) vaccines violates the spirit and principles of the Nuremburg Code.
- Some medical ethicists will argue that the current vaccines are not experimental and that the Nuremburg Code does not apply. However, as laid out in the arguments of this document, there are no long-term studies on the use of synthetic mRNA to treat disease, and forcing the use of this novel therapeutic intervention with the general populace (particularly against the will of any given individual), in my opinion, is an abuse of power.
- Moderna has a long-term goal of curing disease by developing a generic DNA based platform (28) . Scientific critics have acknowledged the impressive nature of such a project, yet note that “the manipulation of the code of life could lead to completely unanticipated negative effects, potentially long term or even permanent” (p. 43, Seneff &.Nigh, 2021).
- Anyone familiar with the history of vaccines, realizes that tragic failures have occurred repeatedly over time, especially when we have rushed vaccine development (see CDC website – for a list of historical concerns in the modern era: https://www.cdc.gov/vaccinesafety/concerns/concerns-history.html).
- The first USA manufactured polio vaccine actually led to accidentally infecting 40,000 children with polio during the 1950s (the Cutter incident) (29).
- The swine flu vaccine of 1976 led to the development of Guillain-Barré syndrome in more than 450 individuals (30, 31). This incident led to the discontinuation of the vaccine, but seems less problematic than current side effect reported with the mRNA and vector-based vaccines.
- In 2017, a school-based dengue fever vaccination program was discontinued in the Philippines after complications and several deaths were linked to a drug called Dengvaxia. This vaccine reportedly increased the risk that a child would contract a more severe form of the disease.
- Outbreak of polio was caused by a failed vaccine campaign by the WHO in Africa in 2020 resulting in permanent paralysis in some Sudanese children (32).
- Will granting approval by the Food and Drug Administration (FDA) finally settle the science? Of course not!
- Approval can only be based on the data in hand. The FDA will watch the effects of these vaccine over time, and their only history warns us that something deemed safe initially may be removed down the road (sometimes after many years of use by the American people.
- Withdrawal of Merck’s Vioxx – This nonsteroidal anti-inflammatory (NSIAD) painkiller had been FDA approved, but was eventually voluntarily withdrawn by the company following reports of increased rates of strokes and heart attacks in patients using this medication on a chronic basis
- Bextra – Another NSIAD pain killer that was ultimately dropped due to two short-term studies which showed an increased risk of cardiovascular events, such as heart attacks and strokes.
- Cylert – Abbott withdrew this drug during 2005 (introduced during 1975) once used to treat Attention Deficit Hyperactivity Disorder (ADHD) after the FDA identified 13 reports of liver failure, which led to either liver transplant or death. The rate of liver failure was 10-25 times greater than that seen in the healthy adult population.
- Approval can only be based on the data in hand. The FDA will watch the effects of these vaccine over time, and their only history warns us that something deemed safe initially may be removed down the road (sometimes after many years of use by the American people.
- Resistance to vaccination has been the subject of much speculation among the media and our political elites, yet there are several interesting patterns worth noting.
- A large survey out of Carnegie Mellon University (more than 5 million respondents to an online survey) showed that vaccine hesitancy was greatest among the young (ages 18 to 24 years), persons with Ph.D.s (particularly if they had already had COVID-19), non-Asian individuals, and less educated respondents. There was a “U-shaped” distribution with those with Ph.D.s and those with less than a high school education being most reluctant to get the vaccine (33).
And finally, Nobel Prize winner Luc Montagnier has expressed strong concerns about the COVID vaccine’s mid-term, long-term, and even generational consequences, and has warned that it is unwise to force vaccination on individuals who are at low risk of severe complications. In an interview with Pierre Barnérias of the French Hold-Up Media earlier this year, Dr. Montagnier made the claim that the COVID-19 vaccines are actually contributing to the rise of variants. He also indicated that epidemiologists know but are “silent” about the phenomenon, known as “Antibody-Dependent Enhancement” (ADE).
Mass vaccinations are a scientific error as well as a medical error. It is an unacceptable mistake. The history books will show that, because it is the vaccination that is creating the variants.”
Nobel Prize winner Luc Montagnier, May 2021
Dr. Montagnier, who won the Nobel prize in Medicine during 2008 for his work related to the discovery of the AIDs virus, has insisted that the SARS-CoV-2 was developed and not a naturally occurring virus. The French free-to-air news channel CNews reported that Dr. Montagnier stated:
“The Wuhan city laboratory has specialized in these coronaviruses since the early 2000s. They have expertise in this area,” he says. The professor explains having analyzed “in the smallest details” the sequence with his mathematician colleague Jean-Claude Perrez. “We were not the first, since a group of Indian researchers tried to publish a study which shows that the complete genome of this coronavirus [has] sequences of another virus, which is HIV, the virus AIDS.”
Dr. Montagnier made his statement after the Indian research group had to retract its publication due to public outcry. He asserted that “scientific truth always ends up emerging,” and noted that he felt the HIV sequence was inserted into the genome of the coronavirus in an attempt to make an HIV vaccine. “It is the work of a sorcerer’s apprentice.”
Although no consensus exists, multiple credible physicians and scientists have drawn similar conclusions about the virus.
References:
- Dan JM, Mateus J, Kato Y, Hastie KM, Yu ED, Faliti CE, et al. Immunological memory to SARS-CoV-2 assessed for up to 8 months after infection. Science. epub.
- Turner JS, Kim W, Kalaidina E, Goss CW, Rauseo AM, Schmitz AJ, et al. SARS-CoV-2 infection induces long-lived bone marrow plasma cells in humans. Nature. 2021;595:421-5.
- Wang Z, Muecksch F, Schaefer-Babajew D, Finkin S, Viant C, Gaebler C, et al. Naturally enhanced neutralizing breadth against SARS-CoV-2 one year after infection. Nature. 2021;595:426-31.
- Zuo J, Dowell AC, Pearce H, Verma K, Long HM, Begum J, et al. Robust SARS-CoV-2 specific T cell immunity is maintained at 6 months following primary infection. Nature Immunology. 2021;22(620-626).
- Goldberg Y, Mandel M, Woodbridge Y, Fluss R, Novikov I, Yaari R, et al. Protection of previous SARS-CoV-2 infection is similar to that of BNT182b2 vaccine protection: A three-month nationwide experience from Israel. medRxiv. 2021.
- Brown CM, Vostok J, Johnson H, Burns M, Gharpure R, Sami S, et al. Outbreak of SARS-CoV-2 infections, including COVID-19 vaccine breakthrough infections, associated with large public gatherings – Barnstable county, Massachusetts, July 2021. In: Prevention CfDCa, editor. Morbidity and Mortality Weekly Report2021. p. 1059-62.
- Cohen KW, Linderman SL, Moodie Z, Czartoski J, Lai L, Mantus G, et al. Longitudinal analysis shows durable broad immune memory after SARS-CoV-2 infection with persisting antibody responses and memory B and T cells. . Cell Reports Medicine. 2021;2(7):100354.
- Shrestha NK, Burke PC, Nowacki AS, Terpeluk P, Gordon SM. Necessity of COVID-19 vaccination in previously infected individuals. medRxiv. 2021.
- Yu X, Tsibane T, McGraw PA, House FS, Keefer CJ, Hicar MD, et al. Neutralizing antibodies derived from the B cells of 1918 influenza pandemic survivoers. Nature. 2008;455:532-6.
- Le Bert N, Tan AT, Kunasegaran K. SARS-CoV-2-specific T cell immunity in cases of COVID-19 and SARS, and uninfected controls. Nature. 2020;584:457-62.
- Majdoubi A, Michalski C, O’Connell SE, Dada S, Narpala S, Gelinas J, et al. A majority of uninfected adults show preexisting antibody reactivity against SARS-CoV-2. The Journal of Clinical Investigation Insight. 2021;6(8):e146316.
- Loyal L, Braun J, Henze L, Kruse B, Dingeldey M, Reimer U, et al. Cross-reactive CD4+ T cells enhance SARS-CoV-2 immune responses upon infection and vaccination. medRxiv. 2021.
- Quadeer AA, Ahmed SF, McKay MR. Landscape of epitopes targeted by T cells in 852 individuals recovered from COVID-19: Meta-analysis, immuoprevalence, and web platform. Cell Reports Medicine. 2021;2(6):100312.
- Girardot M. Natural immunity vs. Covid-19 vaccine-induced immunity. BizNews. 2021.
- Lozano-Ojalvo D, Camara C, Lopez-Granados E, Nozal P, del Pino-Molina L, Bravo-Gallego Y, et al. Differential effects of the second SARS-CoV-2 mRNA vaccine dose on T cell immunity in naive and COVID-19 recovered individuals. Cell Press. 2021.
- Seneff S, Nigh G. Worse than the disease? Reviewing some possible unintended consequences of the mRNA vaccines against COVID-19. International Journal of Vaccine Theory, Practice, and Research. 2021;2 (1):38-79.
- Young R, Bekele T, Gunn A, Chapman N, Chowdhary V, Corrigan K, et al. Developing new health technologies for neglected diseases: A pipeline porfolio review and cost model Gates Open Research. 2018;2:23.
- Doshi P. Will COVID-19 vaccines save lives? Current trials aren’t desitned to tell us. British Medical Journal. 2020;371:m4037.
- Lila AS, :Shimizu AT, Ishida T. PEGylation and Anti-PEG antibodies. Engineering of Biomaterials for Drug Delivery Systems. 2018:51-68.
- Mohamde M, Lila AS, Shimizu T, Alaaeldin E, Hussien A, Sarhan HA, et al. PEGylated liposomes: Immunological responses. Science and Technology of Advanced Materials. 2019;20(1):710-24.
- Ganson NJ, Povsic TJ, Sullenger BA, Alexander JH, Zelenkofske SL, Sailstad JM, et al. Pre-existing anti-polyethylene glcol antibody linked to first-exposure allergic reactions to pegnivacogin, a PEGylated RNA aptamer. The Journal of Allergy and Clinical Immunology. 2016;137(5):1610-3.
- Lee SH, Cha JM, Lee JI, Joo KR, Shin HP, Baek IH, et al. Anaphylactic shock caused by ingestion of Polyethylene Glycol. Intestinal Research. 2015;13(1):90-4.
- Povsic TJ, Lawrence MG, Lincoff AM, Adkinson NF, Levinson AM, Investigators obotR-P. Pre-existing anti-PET antibodies are associated with severe immediate allergic reactions to pegnivacogin, a PEGylated aptamer. The Journal of Allergy and Clinical Immunology. 2016;138(6):1712-5.
- Kelso JM. Anaphylactic reactions to novel mRNA SARS-CoV-2/COVID-19 vaccines. Vaccine. 2021;39(6):865-7.
- Health NIo. NIH-Moderna COVID-19 vaccine shows promising interim results NIH Record2020 [cited 2021.
- Maramattom BV, Krishnan P, Paul R, Padmanabhan S, N’ampoothiri SCV, Syed AA, et al. Guillain-Barre syndrome following ChAdOx1-S/nCoV-19 vaccine. Annals of Neurology. 2021;90(2):312-4.
- Allen CM, Ramsamy S, Tarr AW, Tighe PJ, Irving WL, Tanasescu R, et al. Guillain-Barre syndrome variant occurring after SARS-CoV-2 vaccination. Annals of Neurology. 2021;90(2):315-8.
- Moderna. mRNA platform: Enabling drug discovery and development 2020.
- Fitzpatrick M. The Cutter incident: How America’s first polio vaccine led to a growing vaccine crisis. Journal of the Royal Society of Medicine. 2006;99(3):156.
- Krause R. The Swine Flu episode and the fog of epidemics. Emergent Infectious Diseases. 2006;12(1):40-3.
- Dehner G. WHO knows best?: Nationa and international responses to pandemic threats and the “lessons” of 1976. Journral of the History of Medicine and Allied Sciences 2010;65(4):478-513.
- Cheng M. UN says new polio outbreak in Sudan caused by oral vaccine. AP News. 2020 September 2, 2020.
- King WC, Rubinstein M, Reinhart A, Mejia RJ. Time trends and factors related to COVID-19 vaccine hesitancy from January-May 2021 among US adults: Findings from a large-scale national survey. medRxiv. 2021.